
There are very good reasons why many infectious disease experts spend a lot of time focused on the threat of influenza. This virus is a known pandemic threat and has producing such devastating phenomenon at regular intervals throughout human history.
Our chief means of defense against this threat -- as it is with almost all infectious disease threats -- is vaccination. However, as I and many others have written, we largely battle flu with a vaccine technology from the 1940s that has many limitations and at best is possibly about 60% protective and its worst not so protective at all.
Influenza is a tricky virus and has the capacity to drift, shift, mutate, and reassort in a manner that renders vaccines obsolete and requires an intensive process of regular reformulation (because we do not have a universal evergreen flu vaccine). This process is further complicated because the vaccine is grown in chicken eggs -- a cumbersome process that not only is dependent on a supply of chicken eggs but can itself mutate the vaccine strain during growth further handicapping the vaccine.
One solution to this problem is to move out of chicken eggs altogether and to cell lines -- something that is the norm for many other vaccines. To date, however, only one totally cell-based vaccine is available (there is another partial cell-based vaccine as well which relies on an egg derived viral reference strains that is then grown in MDCK cells): Flublok, a recombinant vaccine grown in insect cells through a baculovirus vector.
It's no secret that I am a huge fan of this vaccine, insisted on receiving it this season, recommend it to my friends, and even got to tour their vaccine plant. The value of FluBlok is not only that it frees flu vaccine production from the tyranny of eggs from a production standpoint, but that its recombinant nature results in a better vaccine. A recent study, published in The New England Journal of Medicine, illustrates this latter point.
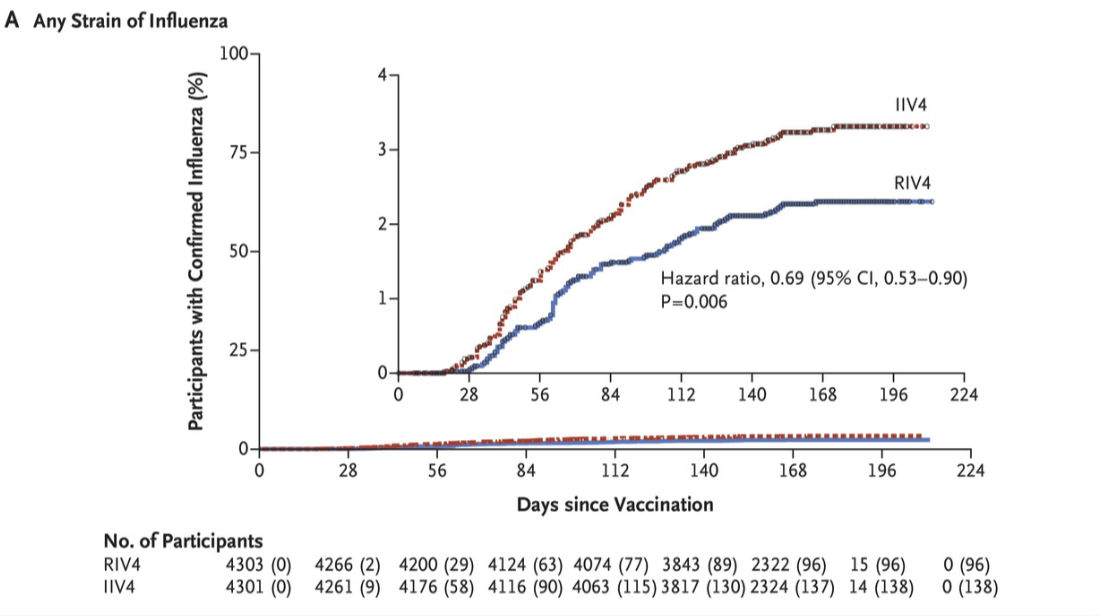
During the 2014-2015 influenza season -- a season characterized by influenza A/H3N2 dominance and vaccine mismatch-- a randomized clinical trial was conducted on 9000 individuals aged 50 years of age and older. Participants were randomized to quadrivalent FluBlok vs. a standard quadrivalent GSK flu vaccine. The primary endpoint was PCR confirmed influenza-like illness.
Fully 30% less participants randomized to FluBlok experienced PCR-positive influenza reaching statistical superiority. In subgroup analysis, this appeared to be derived from enhanced protection against influenza A. Since no influenza A/H1N1 was detected in the study, the result was driven from enhanced efficacy against A/H3N2 -- a usually more severe strain of seasonal flu. No safety concerns arose.
This trial is very significant and should help physicians and the public understand that moving away from eggs in vaccine production will have many important effects including rapid scale up, flexibility in plugging in new strains of flu and other viruses (e.g. Zika), and no susceptibility to egg supply shocks (a real concern during an avian flu outbreak that could make chicken egg supplies dwindle), less mutation of vaccine strains induced by adaptation to egg growth, and -- as this trial illustrates -- better protection during seasonal flu.



